Urinary Stone
On an average, lifetime prevalence of stone disease ranges from 1% to 15%. Relatively rare below 20 years of age, it is two to three times more common in men than in women. High prevalence is seen in hot, arid and dry climates (mountains, deserts and tropical areas. In India, stone disease is more common in Northern part and in Deccan plateau. Seasonal variation is seen with highest incidence in summer months. Risk also increases with body weight
Three-fourth of all stones contain calcium, which makes it visible in the x-rays. Calcium oxalate is the predominant stone variant (93% in India). Non-calcium stones are like struvite (infection stone) and uric acid stone. Uric acid stone is not visible in plain x-ray, but can be visualized in CT scan.
How can we suspect stone disease?
Stones most commonly present as excruciating pain, starting from flank region and going down to groin or genitalia. The patient may feel nauseated or even vomit. The sufferer fails to get any relief, as he tosses around in the bed. This may be associated with burning sensation when attempting to void, frequent voiding with little amount of urine, occasional blood in urine. Any episode of fever with chills is a dangerous sign of infection.
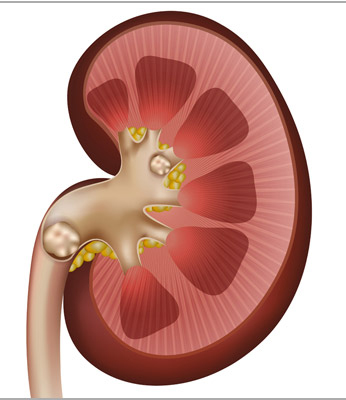
Occasionally, the stones may silently damage the kidney. Sometimes, the stone may block the drainage from the kidney, leading to hydronephrosis (swelling in the kidney) and in extreme case, complete loss of kidney mass.
How is the diagnosis of stone disease made?
Suspicious history or sometimes non-specific abdominal pain leads to investigation with detection of stones. Stones more than few mm size can be picked up by ultrasound and X-rays. Both these techniques have their own technical limitations with chances of missing the stone. Plain CT of abdomen is up to 98% accurate in detecting even the smallest of stones, including those not seen on X-rays. The patient needs specialized radiological tests like IVP or CT-IVP for proper evaluation before any surgical intervention.